
The C-reactive protein (CRP) test is widely used in the Nordic countries and high CRP values are frequently seen in bacterial infections. However, slightly increased CRP levels can be difficult to interpret and there are also non-bacterial diseases that might cause elevated levels. This may mislead clinicians in the decision to prescribe antibiotics.1
White blood cells (WBC) are rapidly released from the bone marrow at the onset of fever, as part of the acute phase response to an infection. Using a WBC count as a complement to CRP can substantially increase the detection rate of bacterial infections.2 In addition, a WBC count may be clinically relevant for other conditions than just infections/inflammations, e.g., suspected hematological malignancies, toxic marrow suppressions, unexplained and severe anemia.3
HemoCue® WBC DIFF System provides a white blood cell count with a 5-part differential in just 5 minutes. Access to a WBC count at the point of care may help you to:
- Distinguish between viral and bacterial infections
- Keep judicious use of antibiotics
- Rule out serious conditions
Want to learn more about WBC point-of-care testing? Fill in the form to get in touch!
Want to learn more about WBC point-of-care testing?
Publications for download
Discrepancy between total white blood cell counts and serum C-reactive protein levels in febrile children
WBC and CRP are commonly discrepant in febrile children and measuring both markers substantially increases the detection rate of bacterial infection. The value of measuring both markers is supported by two findings. First, in a substantial proportion of children with severe bacterial-type diseases only one of either CRP and WBC is increased. Secondly, elevation of both parameters signifies a high risk of bacterial disease.
The course of C-reactive protein response in untreated upper respiratory tract infection
High CRP values are frequently seen in bacterial infections, but elevated values are also seen in viral respiratory infections, and peak values have been demonstrated 2-4 days after viral challenge.
Neutrophil to lymphocyte count ratio as a biomarker of bacterial infections
The result from this study suggest diagnostic potential of NLCR that may serve as a simple marker for discrimination between severe bacterial and viral infections. Direct availability, low cost, and high reliability of the NLCR support its incorporation into routine diagnostic panels.
Comparison of C-Reactive Protein (CRP) and White Blood Cell (WBC)
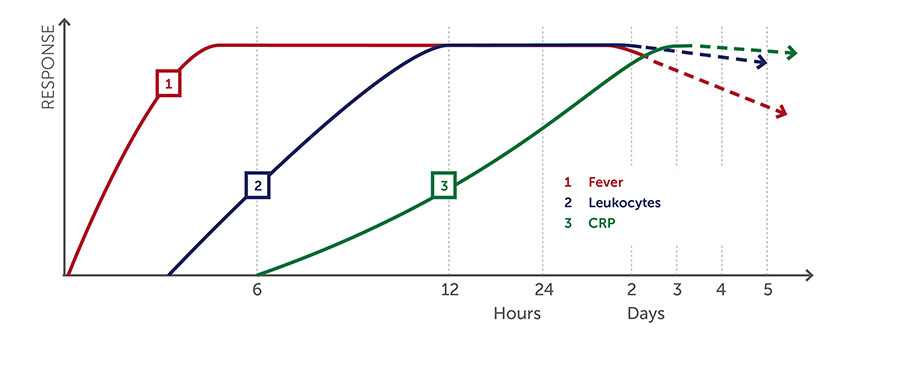
- Both CRP and WBC are used as inflammatory/infection markers. CRP and WBC react differently over time and with different clinical conditions. WBC is rapidly increased at the onset of fever, whereas CRP peaks in ~2-4 days. Using both markers can increase detection of bacterial infections.1-2
- Slightly increased CRP levels can be difficult to interpret and there are also non-bacterial diseases that might cause high CRP levels. This may mislead clinicians in the decision to prescribe antibiotics.1
- A WBC count may be clinically relevant for other conditions than just infections/inflammations, e.g., suspected hematological malignancies, toxic marrow suppressions, unexplained and severe anemia.3
WBC vs CRP onset during bacterial infections
White blood cell count (WBC) in general, responds more rapidly to bacterial infections with fever compared with C-reactive protein (CRP). The two markers are complementary to each other, and measuring both could potentially increase the detection rate of bacterial infections, as well as ensuring appropriate initiation of antibiotic treatment.
*The graph is a schematic interpretation of WBC vs CRP onset based on data from several publications.
1. Melbye H et al. The course of C-reactive protein response in untreated upper respiratory tract infection. Br J Gen Pract. 2004 Sep;54(506):653-8.
2. Peltola et al. Discrepancy between total white blood cell counts and serum C-reactive protein levels in febrile children. Scandinavian Journal of Infectious Diseases. 2007; 39:560-565.
3. Laurells Klinisk Kemi i praktisk medicin (Laurell’s Clinical Chemistry in Practical Chemistry), 2003, 8th edition.

A white blood cell differential count can bring you closer to a conslusive answer in many situations. It can help you determine whether an infection is viral or bacterial. It can help you monitor a patient’s response to treatment. And in situations with unspecific symptoms, such as fever or fatigue, it can direct you in terms or further testing and treatment steps. See how the system is being used in a couple of primary care centers in Sweden.

HemoCue® WBC DIFF System provides a quantitative total white blood cell count with a 5-part differential right at the point of care.
- Results in just 5 minutes
- Easy to use by healthcare professionals
- 10uL of capillary or venous whole blood
HemoCue has been a leader in Hb point-of-care medical diagnostics for over 40 years. We specialize in giving healthcare providers lab-quality results comparable to that of a clinical lab.
HemoCue AB
Kuvettgatan 1
SE-262 71
Ängelholm
Sweden
Phone: +46 77 570 02 10
Email: [email protected]
Website: www.hemocue.com
 White blood cell count provides valuable information in the diagnosis or exclusion of an infection. Based on HemoCue’s microcuvette technology, the WBC system allows medical professionals to accurately determine total white blood cell counts right at the point of care.
White blood cell count provides valuable information in the diagnosis or exclusion of an infection. Based on HemoCue’s microcuvette technology, the WBC system allows medical professionals to accurately determine total white blood cell counts right at the point of care. The WHO called for reducing anemia by 50% in women of reproductive age, as part of its 2025 World Health Assembly Global Nutrition Targets. This made the assessment of anemia a global priority, and at HemoCue, we knew that we could make a difference. We launched
The WHO called for reducing anemia by 50% in women of reproductive age, as part of its 2025 World Health Assembly Global Nutrition Targets. This made the assessment of anemia a global priority, and at HemoCue, we knew that we could make a difference. We launched